What Causes Insomnia? Identifying Your Sleep Triggers
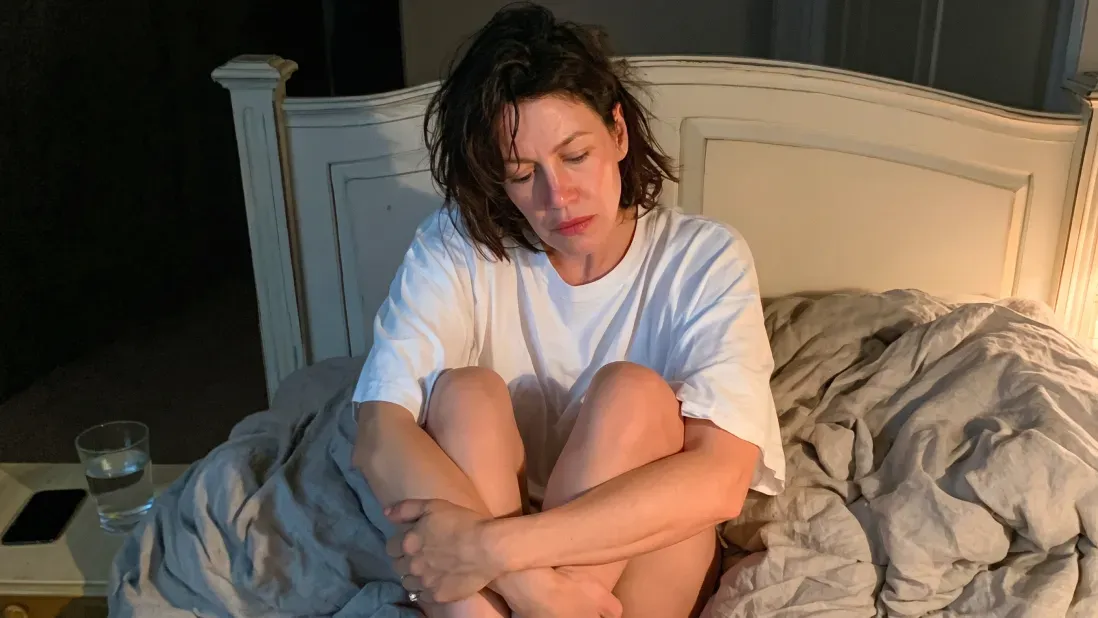




We all have occasional nights where sleep feels out of reach. But sometimes, that one sleepless night slips into a week, and suddenly, days have turned into months of constant, draining exhaustion. Even after eight hours in bed, you wake up feeling as though you’ve barely rested.
That’s chronic insomnia, and 16% of adults worldwide, over 850 million people, are living with it.
Because insomnia is a distinct medical condition linked to serious risks like heart disease, it's worth knowing whether you're facing a temporary slump or a chronic pattern that needs attention.
So, let’s dig deeper into what is sabotaging your sleep.
Key Learnings
- Chronic stress keeps your nervous system in a fight-or-flight state that is physically incompatible with sleep.
- Comorbid insomnia is frequently a symptom of underlying physical issues like apnea or RLS that require medical treatment.
- Many common prescriptions can disrupt neurotransmitters or sleep cycles, often leading to acute insomnia.
- Maintaining a sleep journal and mood tracker helps you identify the specific patterns connecting your daytime stress to your nighttime restlessness.
4 Factors That Can Cause Insomnia
To understand why insomnia takes hold, it helps to view it through the 3 Ps model, a framework sleep specialists use to explain how sleep problems evolve:
- Predisposing factors: These are the vulnerabilities you were born with, like your genetics, age, or being a naturally short sleeper. These don't cause insomnia on their own, but they lower your threshold for it.
- Precipitating factors: These are the triggers that start the problem, like a death in the family, a high-stress job, or a medical crisis.
- Perpetuating factors: These are the habits you adopt to fix the problem. This includes taking long naps, drinking alcohol to wind down, or watching the clock.
Here are the ways these factors manifest in your daily life, whether that's difficulty falling asleep or feeling tired despite a full night's sleep.
Psychological and Emotional Stress
The most common cause of insomnia is hyperarousal, and this is rooted in how the brain’s emotion and threat-detection systems behave. Sleep starts when your system powers down. Your heart rate drops, brain activity slows, and attention to the outside world fades.
When you’re stressed, cortisol increases, and that shutdown doesn’t happen. Your brain and nervous system can stay switched on, lingering in a state of high alert long after you'd like them to power down. So even if you’re tired, your brain isn’t fully letting you sleep. This is also why even if you might fall asleep early, you wake up often or feel restless.
This is a loop. Bad sleep makes it harder for your brain to process stress overnight. That means more emotional reactivity the next day, which keeps the system activated again at night. Lifestyle and Behavioral Habits
Similarly, long-term insomnia raises the risk of depression and anxiety, and those conditions feed right back into the same hyperarousal that keeps you awake, worsening your insomnia.
Medical Conditions and Physical Pain
Sometimes, insomnia is a symptom of a larger, untreated problem. You might think you have "trouble sleeping," but in reality, your body is being pulled out of rest by an underlying issue. Some common causes are:
- Obstructive sleep apnea
- Restless Leg Syndrome (RLS)
- Gastroesophageal reflux (GERD)
- Nightmare disorders
For many women during menopause, hormonal shifts, specifically the decline in estrogen combined with hot flashes, can also create a direct physiological barrier to maintaining sleep. Similarly, during pregnancy, hormonal changes, fetal movement, bladder pressure, physical pain, and heartburn can all result in acute insomnia. For some people, sleep gets better once the underlying issue is treated. For others, insomnia takes on a life of its own and lingers as its own chronic pattern, even after the original cause is gone.
Medication Side Effects
It is easy to focus on lifestyle or stress while ignoring the chemical impact of your medicine cabinet. Some commonly prescribed medications can interfere with the systems that govern your sleep and how easily your body winds down.
- SSRIs (Antidepressants): SSRIs work by boosting serotonin activity in the brain, which can ease the weight of depression and anxiety. However, many SSRIs can have an activating effect on the central nervous system, particularly when you first start taking them. This means you might take longer to fall asleep.
- Corticosteroids: Drugs like prednisone act as powerful cortisol mimetics, which is why glucocorticoids can disrupt sleep, especially at higher doses. Since cortisol is your body’s primary wake-up hormone, these medications effectively trick your nervous system into thinking it is daytime. If taken later in the day, they keep your HPA axis (the stress-response system) in a high-alert state, making it nearly impossible to drift off.
- Beta-blockers: Prescribed for high blood pressure, these medications may inhibit melatonin production, the hormone that signals your brain that the sun has set. Without that biological signal, you may feel physically tired but mentally wired.
Note: If your sleep problems started right after you began a new medication, always consult your doctor before stopping the medication.
Bad Sleep Habits
Finally, your bedtime routine acts as a collection of cues that tell your brain whether it is time to be alert or to shut down. If these signals are misaligned with your biology, you are effectively fighting your own circadian rhythm.
- Temperature: Your sleep cycle is tied to your body's core temperature. To fall asleep, it has to drop by roughly 1-2°F, and a too-warm bedroom makes it harder for your body to shed that heat.
- Light: Light is the most powerful zeitgeber (time-giver) for your internal clock. Even low levels of ambient light can suppress melatonin production by signaling the suprachiasmatic nucleus (SCN) (the brain’s master clock) that it is still daytime. This is also why doctors advise you to avoid screens and blue light before bedtime.
- Conditioning: The brain works on patterns. If you spend long periods awake in bed, you inadvertently train your brain to associate the bed with frustration, screen time, or work, rather than sleep.
- Drinks: What you consume impacts your sleep architecture. Caffeine blocks sleep pressure, keeping you alert, while alcohol, despite making you feel drowsy, fragments your sleep cycle and prevents you from reaching deep sleep.





The Clinical Threshold for Insomnia
Let’s start by defining the line between a rough week and a clinical issue. A simple test is the 3x3 benchmark. If you've been struggling to fall asleep, staying asleep, or waking too early at least 3 nights a week for three months or more, and it's wearing on your days, that may point to chronic insomnia.
Particularly if it is resulting in a daytime tax.
So even if you don’t feel any immediate effects, over time, your body and mind will slow down.
Diagnosing Insomnia
Getting to the bottom of sleep issues usually involves a three-step process to identify what is preventing you from resting.
1. The clinical interview
Your doctor will review your sleep history, typical sleep duration, and substance use. This is a direct conversation about your daily routine, including the timing of caffeine, alcohol, and any medications you are taking. Being honest about these habits is essential, as they often play a major role in how your brain chemistry regulates sleep.
2. A two-week sleep diary
It is difficult to accurately assess your sleep when you are exhausted. Keeping a diary provides the data needed to see the patterns you might miss. You will track your bedtime, how long it takes you to fall asleep, how often you wake, and your caffeine or alcohol intake.
3. Rule-out testing
Sometimes, sleep difficulties are a symptom of an underlying medical condition rather than behavioral habits. Your doctor may suggest diagnostic testing to determine whether a physical barrier is preventing you from resting. This can be:
- Actigraphy: A wearable device that tracks your rest and activity cycles over several days to provide objective data on your sleep architecture.
- Polysomnography (Sleep Study): An overnight study that monitors brain activity, breathing, and heart rate. This is the standard way to rule out conditions like Obstructive Sleep Apnea (OSA) or Restless Leg Syndrome (RLS), which can physically disrupt your ability to stay asleep.
Find Out What's Driving Your Insomnia
Insomnia usually isn’t caused by just one thing. It’s a combination of factors, e.g., your baseline biology, stress, and habits that feed into one another and keep the problem going. In most cases, it’s a loop and not a single issue you can fix in isolation.
The goal is to figure out what’s driving it. Once you can tell whether it’s coming from your health, your behavior, or your environment, you can focus on the right solution instead of guessing.
References
- Benjafield, A. V., Sert Kuniyoshi, F. H., Malhotra, A., Martin, J. L., Morin, C. M., Maurer, L. F., Cistulli, P. A., Pépin, J.-L., & Wickwire, E. M. (2025). Estimation of the global prevalence and burden of insomnia: A systematic literature review-based analysis. Sleep Medicine Reviews, 82, Article 102121. https://doi.org/10.1016/j.smrv.2025.102121
- Bigalke, J. A., Cleveland, E. L., Barkstrom, E., Gonzalez, J. E., & Carter, J. R. (2023). Core body temperature changes before sleep are associated with nocturnal heart rate variability. Journal of Applied Physiology, 135(1), 136–145. https://doi.org/10.1152/japplphysiol.00020.2023
- Espie, C. A. (2023). Revisiting the psychobiological inhibition model: A conceptual framework for understanding and treating insomnia using cognitive and behavioural therapeutics (CBTx). Journal of Sleep Research, 32(6), Article e13841. https://doi.org/10.1111/jsr.13841
- Kato, T., Okawa, G., Tanaka, K. F., & Mitsukura, Y. (2023). Dexamethasone induces sleep disturbance in a dose-dependent manner in mice. PLOS ONE, 18(12), Article e0296028. https://doi.org/10.1371/journal.pone.0296028
- Matsushita, D., Xiong, X., & Wang, X. (2025). Commuting time, residential floor area, and their associations with insomnia and daytime sleepiness among residents of the Tokyo metropolitan area: A cross-sectional study. Journal of Transport & Health, 44, Article 102156. https://doi.org/10.1016/j.jth.2025.102156
- Van Someren, E. J. W. (2021). Brain mechanisms of insomnia: New perspectives on causes and consequences. Physiological Reviews, 101(3), 995–1046. https://doi.org/10.1152/physrev.00046.2019
- Zhang, X., Sun, Y., Ye, S., Huang, Q., Zheng, R., Li, Z., Yu, F., Zhao, C., Zhang, M., Zhao, G., & Ai, S. (2024). Associations between insomnia and cardiovascular diseases: A meta-review and meta-analysis of observational and Mendelian randomization studies. Journal of Clinical Sleep Medicine, 20(12), 1975–1984. https://doi.org/10.5664/jcsm.11326
FAQ: What Causes Insomnia
What exactly is insomnia?
Why is insomnia happening to me?
How does stress affect my rest?
Are there long-term risks to poor sleep?
What is the best way to treat these insomnia issues?
When should I see a doctor for insomnia?
